Data Drop- SUD Gap Map
The Treatment Gap: States with the Most Drug-Related Foster Care Entries Have the Fewest Treatment Facilities
By Xiayun Tan, PhD
Read it in plain text below, or as a downloadable and printable PDF here
Parental substance use is among the most commonly cited reasons children enter foster care.
Child welfare agencies report persistent difficulties connecting parents with substance use disorder treatment– citing long waitlists, geographic gaps, and limited high-quality providers.
But the scale of that gap has been hard to see. How short is the system on treatment capacity relative to the families who need it?
New data from the 2024 National Substance Use and Mental Health Services Survey and AFCARS makes the pattern visible.
States where caretaker substance use drives the highest share of foster care entries are also the states with the thinnest SUD treatment capacity.
Why Substance Use Now Sits at the Front Door of Foster Care
Caretaker drug use has become a defining feature of today’s foster care system.
The share of foster care entries attributed to caretaker drug use has risen from roughly 15 percent in 2000 to more than 40 percent in 2024– even as total foster care entries have declined since their 2016 peak.
Treating parental drug use not only helps parents recover but also potentially improves child welfare outcomes.
Child welfare agencies have responded by relying more heavily on treatment as a prevention and reunification strategy. In practice, that has meant attempting to connect parents to substance use disorder (SUD) treatment in lieu of removal or as a condition of reunification.
But agencies consistently report the same constraint: treatment is hard to find.
Making the Treatment Gap Visible
Previous efforts to quantify SUD treatment availability have largely focused on a narrow slice of care– most often opioid agonist therapy measured through counts of opioid treatment programs or X-waivered buprenorphine prescribers.
That framing no longer captures the treatment landscape child welfare agencies actually navigate. Clinical practice, financing rules, and federal policy have all shifted.
Medication for Opioid Use Disorder has been expanded to include injectable naltrexone, and the federal X-waiver for buprenorphine prescribing was eliminated in 2023.
More importantly, prior measures rarely ask the key question child welfare systems face: Is treatment capacity aligned with the volume of families entering foster care due to caretaker substance use?
We’re filling this gap by combining 2024 data from the National Substance Use and Mental Health Services Survey (N-SUMHSS) with Adoption and Foster Care Analysis and Reporting System (AFCARS) entry data.
We assess state-level SUD treatment facilities capacity relative to foster care entries involving caretaker drug use at the time of removal.
The analysis focuses on facility counts rather than bed capacity, reflecting limitations in public N-SUMHSS data. States also vary in how caretaker drug use is reported under AFCARS, meaning rising prevalence of caretaker substance use might reflect better reporting in some jurisdictions.
For more details on our approach, see the Methodological Details at the end.
SUD Treatment Capacity Relative to Foster Care is Uneven Nationally
In 2024, nearly 16,000 facilities provided substance use disorder treatment services across the country On average, states had 4.7 SUD treatment facilities per 100,000 residents.
But that national average masks wide state-level variation.
States such as Kentucky (12.9), Alaska (12.2), and Maine (10.7) had the highest number of SUD treatment facilities per 100,000 residents.
At the other end of the spectrum, Texas (1.8), South Carolina (1.9), Alabama (2.9), and Florida (3.0) all reported three or fewer SUD treatment facilities per 100,000 residents.
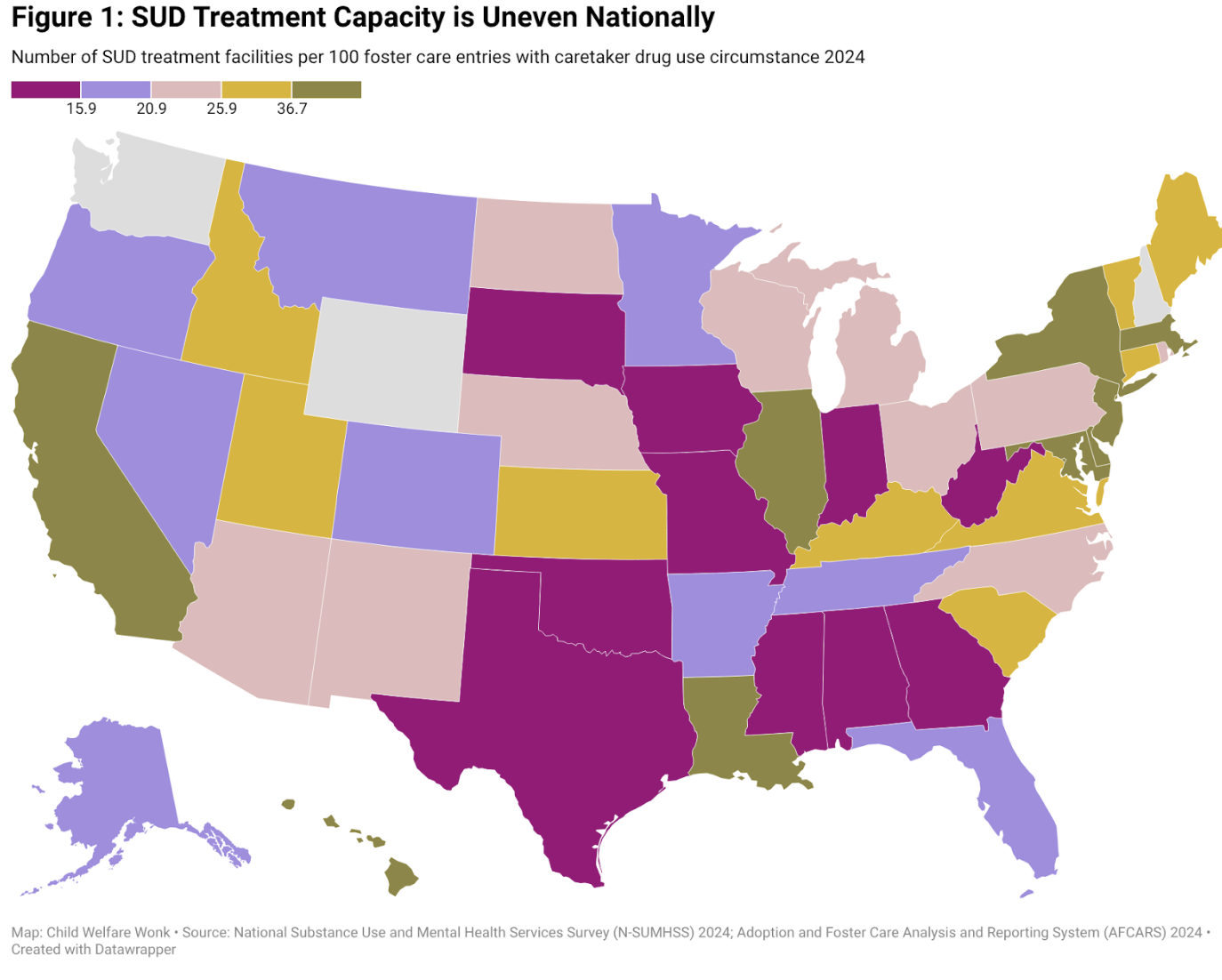
Figure 1 shows SUD treatment capacity measured against foster care entries involving caretaker drug use. Nationally, states averaged 23 SUD treatment facilities per 100 such entries in 2024.
NOTE:Washington and Wyoming did not submit AFCARS 2020 data for FFY2024. New Hampshire did not submit caretaker drug use data. Some wide range of reported information can be the result of variations in jurisdictions' reporting practice. Such outliers do not impact analysis findings.
SUD treatment capacity varied significantly by state, ranging from fewer than 7 SUD treatment facilities per 100 caretaker drug-related entries in Oklahoma to over 300 in Louisiana.
Several states– including California, New Jersey, Delaware, Hawaii, Illinois, Maryland, and Louisiana– reported more than 50 treatment facilities per 100 caretaker drug-related entries.
At the other end of the spectrum, Oklahoma, Texas, West Virginia, and Alabama reported fewer than 10 facilities per 100 such entries– placing them well below the national average.
SUD Treatment Capacity is Lowest Where Need for Treatment is Highest
Nationally, about 40 percent of new foster care entries in 2024 involved caretaker drug use. In several states, that share exceeded half of all new entries.
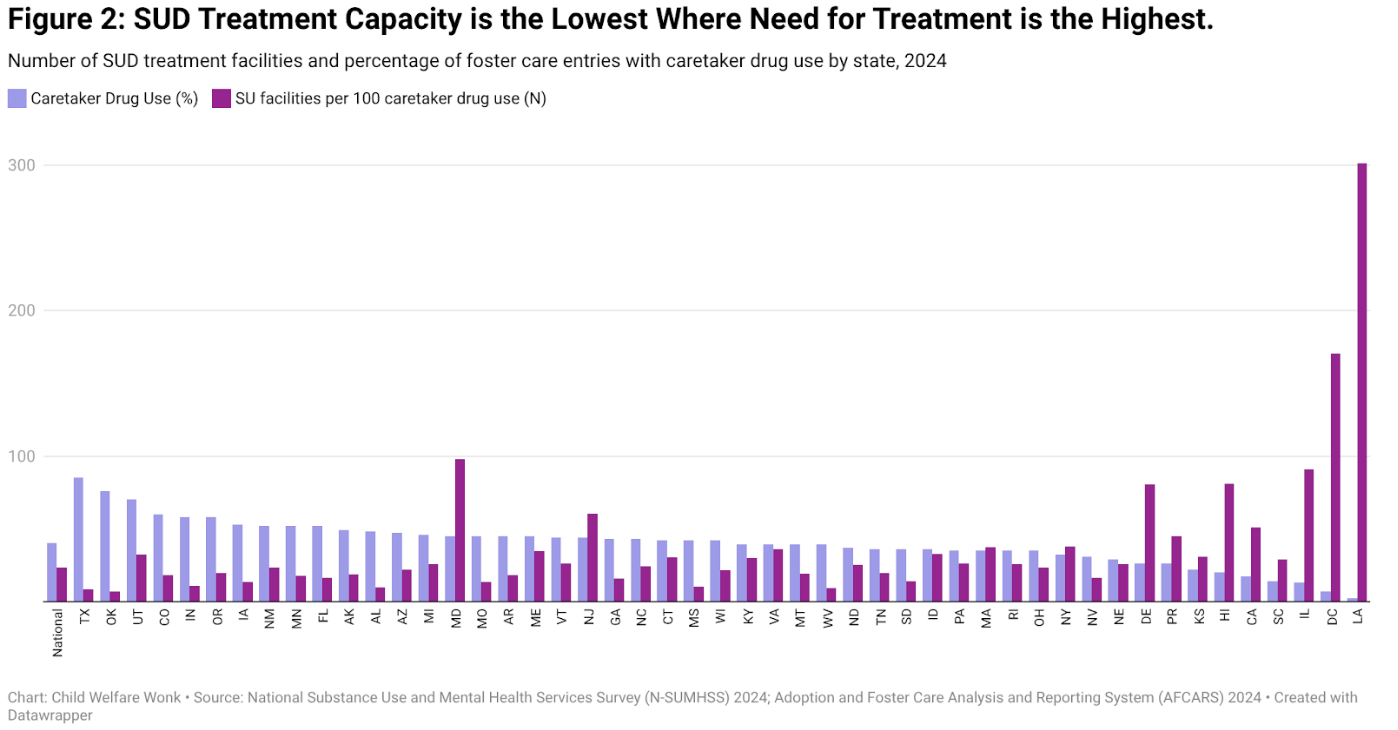
States where caretaker substance use accounted for the largest share of foster care entries consistently reported below-average SUD treatment capacity (Figure 2).
Among the ten states where more than half of the new foster care entries involved caretaker drug use –including Texas, Oklahoma, Utah, Colorado, Indiana, Oregon, Iowa, New Mexico, Minnesota, and Florida–nine (all except Utah) had fewer treatment facilities per caretaker substance-related entry than the national average.
The gap is most pronounced in Texas and Oklahoma.
In 2024, caretaker substance use was cited in 85 percent of new foster care entries in Texas and 75 percent in Oklahoma, yet both states had the lowest SUD treatment capacity nationally.
We also found a significantly strong and negative correlation between SUD treatment capacity and the share of foster care entries involving caretaker substance use (r=-0.59, p=0.00).
This suggests that an increase in SUD treatment capacity would result in a decrease in caretaker drug use prevalence among foster care entries.
What the Capacity Gap Signals for Child Welfare Policy
Our findings reveal a critical mismatch embedded in current child welfare policy. Federal and state systems increasingly rely on SUD treatment as a mechanism to prevent foster care entry and support reunification.
Yet treatment capacity is weakest in the very jurisdictions where caretaker substance use is most likely to drive removal decisions.
This mismatch helps explain why prevention policy often struggles at the point of implementation.
When treatment slots are scarce, geographically distant, or incompatible with parenting requirements, substance use is more likely to translate into foster care entry—even when prevention funding and policy flexibility technically exist.
More broadly, treatment capacity appears to function as a gatekeeper within the child welfare system.
Where capacity is thin, agencies face fewer viable alternatives to placement. Where capacity is stronger, substance use is less likely to be the decisive factor pushing families into foster care.
Understanding this capacity constraint is essential for interpreting foster care entry trends and for assessing the real-world reach of prevention policy.
Without aligning treatment infrastructure with the geography of child welfare needs, expectations for prevention are likely to continue outpacing what systems can deliver.
Methodological Details
This study uses the National Substance Use and Mental Health Services Survey (N-SUMHSS), a comprehensive national source of data on substance use disorder treatment facilities’ geographic location, service provision, and operation characteristics. SU facilities which only provide non-treatment services are excluded from the N-SUMHSS, with the exception of state approved non-treatment substance use halfway houses. Facilities included in the N-SUMHSS treat a wide range of substance use disorders, including but not limited to opioids, benzodiazepines, cocaine, and methamphetamines. Our study uses the number of SUD treatment facilities instead of more detailed facility treatment capacity measurement, such as the bed numbers, because this data is grouped into categories in the public use data files. N-SUMHSS public use data files also do not permit looking into sub-state or urban/rural level information.
Data used in this study is collected under the Adoption and Foster Care Analysis and Reporting System (AFCARS) 2020 final rule (referred to as “AFCARS 2020” data), which features numerous changes to the data elements and reporting format. “AFCARS 2020 data” was first submitted for federal fiscal year (FFY) 2023. The FFY 2024 data used in our study is the second-year submission under the new 2020 rule. Some states are still in a capacity-building phase and there are limitations on some data fields accuracy. For example, under the new “AFCARS 2020” instructions, jurisdictions are required to indicate all circumstances that were present at the time of the child's removal, including the specific reason(s) that a child was removed. However, some states had been reporting only the specific reason(s) for removal. Many states have not trained staff on new definitions and may have not changed their usage.
References
Meinhofer, A., & Angleró-Díaz, Y. (2019). Trends in Foster Care Entry Among Children Removed From Their Homes Because of Parental Drug Use, 2000 to 2017. AMA Pediatr, 173(9), 881-883. doi:10.1001/jamapediatrics.2019.1738